Speaker 1 (00:00):
Every event that we go to, we talk to people who, “How can we accelerate our journey?” We want to have an impact on the device we’re developing, on the people we’re interacting with. This is the thing that gets us excited, which is why we’re here talking about it today, because there’s a tremendous opportunity to have an impact for those who are having an impact on patients. That drives us.
Speaker 2 (00:22):
So that’s what we’re here to talk about today. We’re sharing some of our experiences and advice for how to leverage additive manufacturing responsibly.
Speaker 1 (00:31):
And it’s not as though there’s one right way. The conversation continues to be deep in understanding what are the options out there.
Speaker 2 (00:38):
I think that’s what you should say.
Speaker 1 (00:40):
That’s what I did just say.
Speaker 2 (00:41):
But you looked at me. You were looking down. You need to look up. One of these cameras. Look at this one here.
(00:49):
Welcome to the Solutionology Podcast. Today, we’re going to be talking about scaling additive manufacturing for regulated medical devices. Our mission has always been to provide consistent, high quality production using additive manufacturing, and one of the areas that we started focusing on was medical device, of course, prototyping, but also production.
Speaker 1 (01:13):
In a lot of cases that we serve, there’s an instrument or an installed component of the medical device, and then there’s the rest of the components which are responsible for delivering it or retrieving it or it’s the surgical tools that are used. It’s not the component that’s going in the body, but it’s all OF the stuff that supports the effort to get it there successfully.
Speaker 2 (01:36):
We’re making a distinction. We’re not talking about implantables.
Speaker 1 (01:39):
Yeah.
Speaker 2 (01:39):
We’re talking about the devices that perform the activity on the outside of the body.
(01:45):
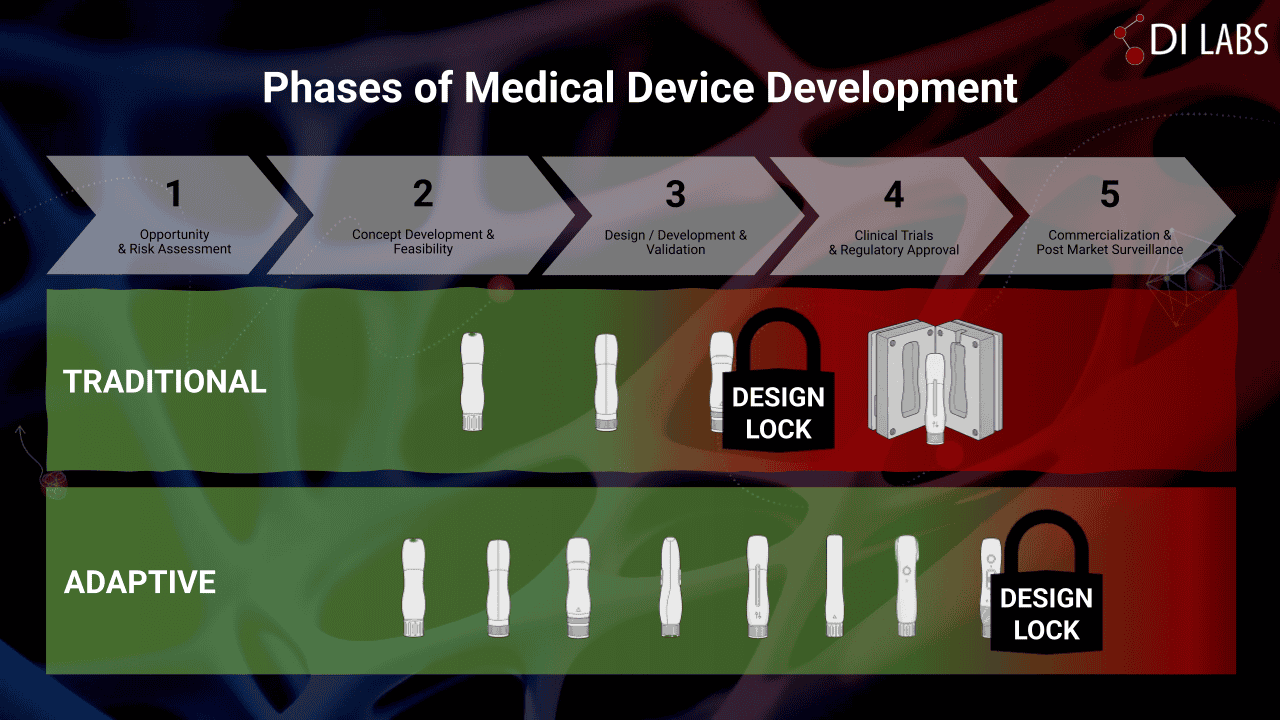
Let’s look at this through the lens of a typical production scenario. Medical devices are heavily prototyped through phase 2 and phase 3. And as you’re going through the phase 3, oftentimes you’re starting to do animal studies, and through that journey, the device optimization improves and the designs become more locked, so that by the end of phase 3, typically the designs are generally locked, with the exception of optimization for human factors. And at that point, that’s where the design history file starts.
(02:24):
Production starts using, for example, injection molding or machining, and then it goes into the clinical trials. And then any changes that are made are part of that design history file for the part and then they roll up to the assembly, and then ultimately it goes to get accepted. But for additive manufacturing, the missing link is the traceability, the dimensional controls. And that’s really what started that journey of internal acceptance. It’s just all about managing risk. So that’s what I think opened the door for additive to go further, migrate further into the process.
Speaker 1 (03:03):
Whether it’s implantable or the surgical device, they’ve all been treated the same. At this end of phase 3, they’re all sort of locked together as a group and they’re treated in a similar way. You have an injection mold, you start to build up your dimensional requirements and tolerance requirements as you go into phase 4, and they’re all sort of carried on in the same approach and there’s no separation.
Speaker 2 (03:26):
So when you say there’s no separation, what’s the significance of that distinction?
Speaker 1 (03:31):
The surgical device or the component that the surgeon’s using during the operation, the flexibility and the functionality of that device, it’s different than the implantable.
Speaker 2 (03:41):
And I think you’re saying is that there’s generally more degrees of freedom on the delivery system than there is on the implantable.
Speaker 1 (03:47):
Yeah.
Speaker 2 (03:48):
And there generally is, and it has a lot to do with the risk. The risk that the device has to cause harm, death in that particular operation, whatever it is.
Speaker 1 (03:59):
So as we think about the traditional sense, having the implantable locked down in the way that is being suggested makes a lot of sense. Until that’s highly controlled and designed, maybe there’s a way to carry that further down the line. But as we think about the devices that help deliver or retrieve or install that implantable, the flexibility of locking that down early, you prevent yourself from having more successful outcomes in clinical trials, or you increase the time upfront to ensure that whatever that you cut or produce is as effective as it needs to be and changes are few and far between.
Speaker 2 (04:37):
Yeah. So one of the challenges of the traditional method where you have 3D printing or additive manufacturing for prototyping, and then you transition to a more traditional method like injection molding, the challenge is, at some point, you’ve got to lock everything down, with the exception of minor optimizations. And that lock nature prevents the application of the learning lessons that happen through the dozens or hundreds in-human clinical trials.
(05:07):
And as we’ve experienced secondhand, those clinical trials are being conducted all across the globe. There’s different mindsets, different approaches, different expectations, and having this one-size solution where you can’t apply those learning lessons from those other regions, and some cases it may prevent improvements in efficacy.
(05:32):
So as we look at this adaptive journey where we’re using additive manufacturing deeper into the development phase, it allows us to go further without locking the designs. Of course, we need the documentation, we need the history files for the designs. We can produce digitally without having to cut a mold, and that allows us the freedom to include human-factor optimizations and other feedback that is achieved from doctors.
Speaker 1 (06:01):
So in a tight timeline scenario where there’s a clinical trial completed and you’re gearing up for the next clinical trial, you may not have the window to go back and do an injection mold change to optimize for some feedback that you had in that first clinical trial. So then you have to move ahead knowing that there’s a tight timeline and only make the changes that you’re allowed to make in order to get to the next one, knowing that you’re leaving some on the table. And what we’ve experienced with additive is that that feedback that occurs in the clinical trial, likely that we can apply adjustments there, test it, verify it, and then release the next production-ready level of files for the next clinical trial to get additional feedback in.
Speaker 2 (06:45):
Which is especially important early in phase 4 where you’ve got a lot of learning to do and you have to go through hundreds of clinical trials. You can see that timeline start to stack up pretty quickly. So this idea of additive, as you’re talking about, it’s like, “Wow, I can get the feedback, I can compile that, I can make design revs, I can test those, validate it, release new production files, and then go to the next clinical trial with these optimized parts.” That’s a dramatic shift from the traditional method.
Speaker 1 (07:20):
In this phase, we may be moving a feature four millimeters or our client may need to adjust something to a small degree to account for something, and an injection mold, some of those small things can be done, but it can be really cumbersome because you have to work all around the tooling that you already have existing and the timeline required to make the changes.
Speaker 2 (07:42):
You just emphasized the fact that we’re not talking about big changes, we’re talking about optimizations, and having that be such a lightweight process from a manufacturing standpoint, there’s no capital involved and there’s no hard time involved, hard time being tooling changes and things like that. Those are eliminated. So the only time is associated with the design time for optimization and then the time to validate that from a pilot run standpoint. And we found doing that results in real improvements.
(08:19):
Well, let’s dive into that. Let’s talk a little bit about what the alternative journey looks like through using additive manufacturing. You’ve got more adaptability, flexibility. How do you manage that?
Speaker 1 (08:32):
By capturing the data.
Speaker 2 (08:36):
But first you got to develop the plan.
Speaker 1 (08:38):
Yeah.
Speaker 2 (08:39):
And that is one of my big fears that gets missed. If you’re going to deploy additive further into the development phases, you’ve got to have that set out almost at the beginning so that everybody knows what to expect, how to manage the files, the design history, and then capture the data, as you’re saying, which is really important, especially in phase 3.
Speaker 1 (09:05):
So the later that you start using additive in a program like this, the less effective it becomes long-term and more traditional the approach will be. And if you start off early on with a plan and you use additive and explore that and see the opportunities for it to be used and how effective it can be and how dimensionally-accurate it can be and how the data collection to ensure that, as we’re making changes down the line, we’re following within the scope that’s required, it can be more valuable in that case, but you have to start early and it has to start with that plan.
Speaker 2 (09:44):
And then making sure that you’re identifying what the critical design features are, critical dimensions are in those parts. You’re communicating that to your manufacturing team, whether that’s in-house or third-party, and then capturing the data of those critical points so that you’re starting to develop a trend of variability and also accuracy.
Speaker 1 (10:07):
And it’d be crazy to think that as some of these devices are coming through, the bomb starts off really large. Maybe it’s 40 components for a device. It’s crazy to think that all those 40 components are going to come out of that process all additively manufactured. Because there’ll be some components in there that are more critical, they have certain material properties or something that we’re not able to produce to. Some of those fall out and they go to injection molding or machining. It’d be crazy to think that they all make it through. So part of that flexibility and the journey is finding the ones that are really important and focusing on them and allowing additive to work its magic.
Speaker 2 (10:49):
So it’s almost like additive gives you more freedom to operate, and because of that, you’ve got to put more controls in place to manage that freedom so that it’s productive and not counterproductive.
Speaker 1 (11:02):
If that’s part of your plan, that all works.
Speaker 2 (11:05):
Right. The key takeaways that I have is that additive can be a powerful resource to improve design optimization, efficacy, and reduce time for even regulated medical devices. That’s awesome. But if you don’t manage it right, it can be a liability. And so if you’re going to use it, make sure you’re intentional about the way that you’re using it and you have a plan in place.
Speaker 1 (11:37):
Having the plan’s important, as I’d have to guess that the experience with an injection mold contractor who’s making a medical device today, I guess that experience there involves a large QC component to make sure that dimensions are tracked, dimensions are done repeatedly, and that has to be the same regardless of manufacturing process. If it’s CNC machining or metal-printed parts or injection-molded parts, that QC component has to be a critical aspect of that manufacturing. If you’re not getting that out of the manufacturing aspect, it doesn’t matter what type of manufacturing you’re doing, that has to be baked into it.
Speaker 2 (12:18):
Yeah. And then right sizing. Right sizing that degree of QC effort for the variability that you can expect in the process, because you’re going to have a different QC process for machining versus injection molding versus additive manufacturing. And additive is probably going to require the most rigorous QC process and AQL for the critical features.
Speaker 1 (12:42):
Yeah. Maintaining good parts.
(12:44):
So we hope that you do reach out to us if you have questions. If there’s anything that we can support on, we’re here to help.